

Stakeholder management in MedTech is not a “soft skill.” It is part of the design-control and risk-control system that determines whether a product can be safely released, adopted, supported, and defended with objective evidence.
This article is MedTech-first and experience-based. In regulated medical software, stakeholder management is not just communication. It is how expectations become testable acceptance criteria, traceable requirements, and approved objective evidence. I share best practices I have seen work in real teams. I also share Failure Patterns (⚠️) that create evidence debt and late rework. For each pattern, I include practical ways to address it.
🧭 TL;DR: In MedTech, stakeholder management is a value and evidence system. It converts competing needs into testable acceptance criteria, traceable requirements, and approved objective evidence. It also sustains alignment across Quality/Regulatory, Clinical, Engineering, Operations, suppliers, and postmarket systems.
How to read
If you’re building MedTech software (SaMD/SiMD), use as a working playbook for evidence-ready stakeholder engagement.
- Start with the operating model: stakeholders as acceptance authorities inside a design-control + risk-control system (Sections 1–2).
- Then the conversion mechanism: Expectation → Evidence, and the loops that keep decisions audit-ready (Sections 3–7).
- Then the standards overlay (optional deep dive): how IEC 62304 implies stakeholder roles via evidence obligations (Section 8).
- Then the PMI compatibility layer: align to PMBOK 8 language without losing the MedTech-first model (Section 10).
- If you implement only one pattern: adopt Expectation → Evidence as your default conversion workflow.
Stakeholders as a control system
Stakeholder management in MedTech
is a control system that turns competing expectations into approved, traceable evidence that can support a safe release.
What it is
If you are new to regulated development, the key shift is simple:
- The team is not only building software.
- The team is building an evidence-backed safety and effectiveness story that has to survive audits, field events, and team changes.

Stakeholders are the people and functions that keep that story coherent. Practically, they do three jobs:
- Define acceptance (what “good” means and what will be accepted)
- identifying who can accept/reject risk and evidence
- Produce and review evidence (what proves it)
- translating needs into objective evidence
- Decide under change (what happens when reality changes)
- governing changes without accumulating uncontrolled evidence debt
Why it exists
In MedTech, a project does not succeed when features ship. It succeeds when you reach release readiness:
- design controls satisfied (requirements → architecture → design → V&V evidence),
- risk acceptability justified (and residual risk accepted by the right decision owners),
- configuration/change control performed,
- training/labeling and operational readiness in place,
- postmarket monitoring and feedback loops ready to catch issues early.
This evidence system is what IEC 62304 enforces for medical device software life cycle processes. It emphasizes traceable requirements, verification and validation, controlled maintenance, configuration management, and problem resolution [1].
Use this chain as the “north star” for the rest of the article:
- Expectation (stakeholder need)
- Agreement (testable acceptance criteria)
- Trace (requirements and links)
- Proof (verification/validation evidence)
- Approval (review + sign-off)
- Release readiness (safe, supportable, defensible)
⚠️ Failure patterns
- “Done” defined as code complete instead of evidence complete
- QA/RA engaged late. Rework increases and schedule slips become structural.
- stakeholder expectations stay verbal → acceptance becomes political
- changes approved without documented impact analysis → traceability breaks, risk file lags, V&V evidence becomes invalid
📜ISO 13485 and ISO 14971
Even when your focus is software and agility, MedTech stakeholder management lives inside two governing systems:
- ISO 13485 / design & development controls: design inputs must translate into outputs. Reviews are required. Verification and validation are required when applicable. Design changes must be controlled and approved. This is the backbone of the “objective evidence” expectation.[4]
- ISO 14971 / risk management: hazards must be identified. Risks must be evaluated. Risk controls must be implemented. Risk controls must be verified for effectiveness. Overall residual risk must be evaluated using objective criteria defined by the manufacturer.[6]
Practical implication: stakeholder engagement is not only alignment. It is how you ensure the right decision owners agree on what counts as adequate evidence and acceptable residual risk. Do this before you lock in architecture, test strategy, and release timing.
Who matters

Stakeholders in MedTech are often acceptance authorities. They are not only an audience for updates.
Rule of Thumb
If a person or group can:
- block a release,
- accept residual risk,
- demand evidence,
- or trigger a CAPA/change,
treat them as a governance stakeholder, not a communications stakeholder.
This aligns with the practical PMI idea that stakeholder engagement is continuous dialogue across the project ecosystem to maintain alignment and credibility [2].
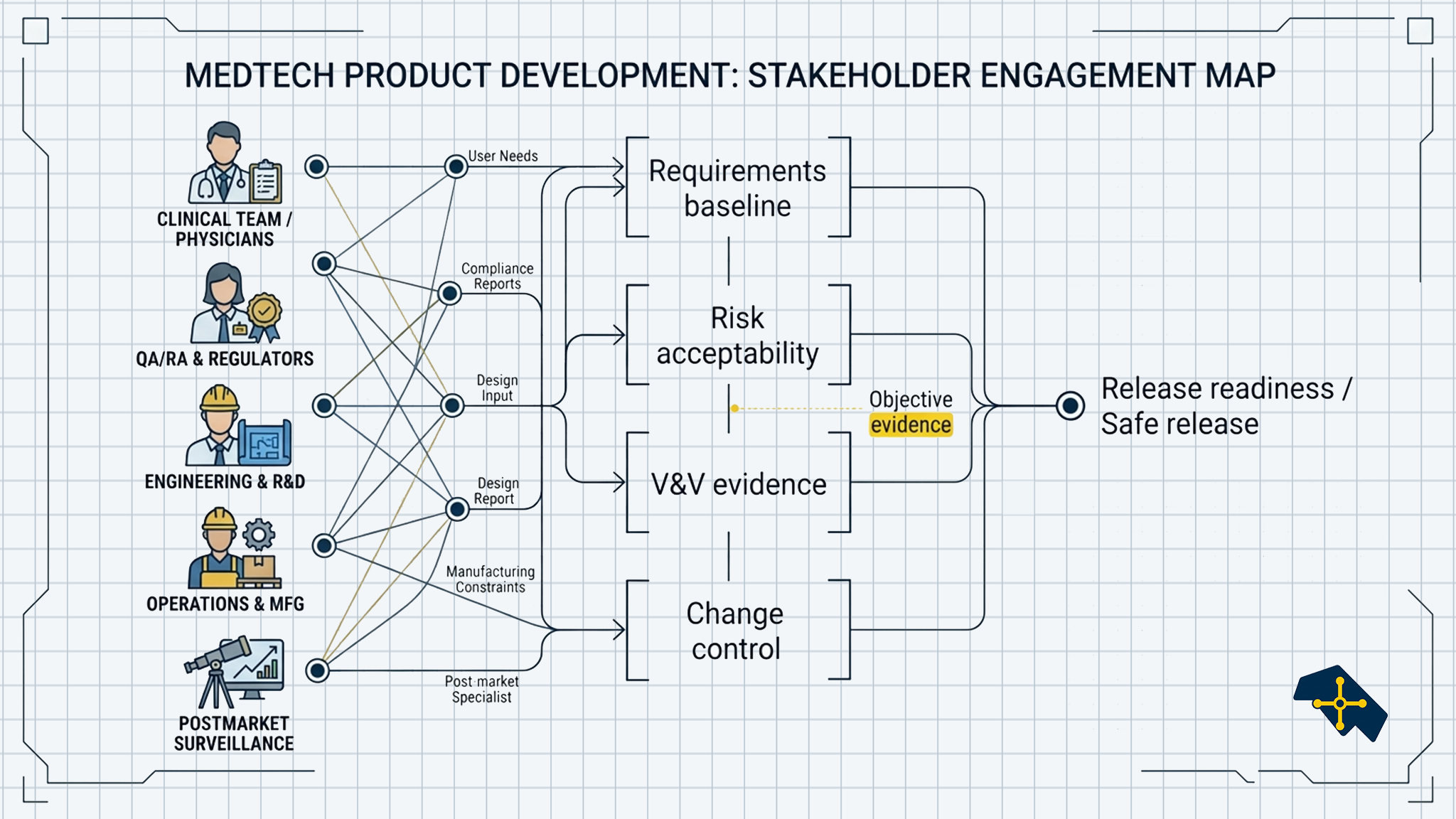
Stakeholder map
Below is a practical “who-to-involve” map. Each group is listed with common sub-stakeholders and what they typically care about or control. This list incorporates implied stakeholders as per IEC 62304 as explained below.
This group defines whether the product “works” in the real world. In MedTech, they often shape usability evidence and acceptance, even if they do not sign formal release gates. They evaluate your workflow fit and shape usability acceptance.
- Who: Clinicians (physicians, nurses, therapists), technicians, biomedical engineers, patients/caregivers (when patient-facing or home-use), clinical informatics / super-users / trainers
- Typical focus: clinical workflow, safety-in-use, usability, alarm burden, documentation burden, adoption
- Typical deliverables to them:
- Workflow walkthroughs and prototypes
- Usability study plan and results summary (as applicable)
- UAT plan, scripts, and feedback log
- Training approach, job aids, and IFU excerpts relevant to use
QA/RA turns “we think it’s ready” into “we can defend it.” They anchor design controls, audit readiness, and the evidence package that supports releases and submissions. 510(k)/PMA/CE technical documentation support.
- Who:
- Design assurance / design control owners (DHF)
- Regulatory affairs (submission-support, technical documentation)
- Document control and training compliance
- Audit readiness / internal auditors
- Typical focus:
- Traceability completeness and DHF integrity
- Design review records and approvals
- Controlled change and configuration baselines
- Evidence quality, consistency, and audit defensibility
- Typical deliverables to them:
- Design and development plans; design review packages and minutes
- Traceability matrix and DHF indexing
- Change request package with impact assessment and approvals
- V&V summary (protocols/reports status, deviations, justification)
Risk owners are acceptance authorities. Their role is to decide what residual risk is acceptable and to ensure risk controls are verified and traceable.
- Who:
- Risk management lead / risk committee members
- Safety officer / clinical safety representatives
- Benefit–risk decision owners (cross-functional)
- Typical focus:
- Hazard analysis quality and completeness
- Risk control adequacy and rationale
- Residual risk acceptability decisions and sign-offs
- Linkage between risk controls, requirements, and verification evidence
- Typical deliverables to them:
- Updated risk analysis with clear hazard sequences and assumptions
- FMEA and/or FTA outputs, when they are part of your chosen risk analysis method
- Risk control list mapped to requirements
- Risk control verification evidence summary (tests/analyses)
- Residual risk rationale and acceptance record
- Updated risk analysis with clear hazard sequences and assumptions
This group produces much of the objective evidence. They also often become a hidden bottleneck when review bandwidth and protocol/report readiness are not planned.
- Who:
- Verification engineers and test leads
- Test automation engineers
- Validation / clinical evaluation support (as applicable)
- Test lab and equipment owners
- Independent reviewers / approvers (when separation is required)
- Typical focus:
- Testability of requirements and acceptance criteria
- Protocol and report quality
- Coverage and regression scope decisions
- Deviation handling and approval timing
- Typical deliverable to them:
- Requirement set with measurable acceptance criteria
- Verification strategy, test plan, and trace links
- Draft protocols early for review; finalized protocols/reports for approval
- Deviation log with disposition and risk/impact justification
Security and privacy stakeholders define constraints that can block release. They also shape what evidence is needed to operate safely and respond to vulnerabilities post-release.
- Who:
- Product security / AppSec
- Security testing and vulnerability management
- Privacy (HIPAA/GDPR), data governance, DPIA owners
- IT / hospital integration stakeholders (SSO, network constraints, firewall rules)
- Typical focus:
- Threat model and security requirements
- SBOM posture and vulnerability response process
- Logging/telemetry and monitoring constraints
- PHI/PII handling, access controls, secure deployment
- Typical deliverable to them:
- Threat model and security requirements set
- SBOM and third-party component inventory
- Security test evidence summary (scans, pen test outputs as applicable)
- Data flow and privacy impact documentation (as applicable)
Engineering (software, systems, hardware) owns feasibility. They translate stakeholder needs into architecture and implementation. In regulated work, they also own the traceable linkage between design decisions and evidence strategy.
- Who:
- Systems engineering (interfaces, allocation, hazard mitigations)
- Software engineering leads and platform teams
- DevOps/SRE / release engineering
- Hardware/firmware (if embedded)
- UX design
- Typical focus:
- Architecture constraints and interface stability
- Performance, maintainability, and safety constraints
- Verification strategy implications of design choices
- Definition of “done” beyond code complete
- Typical deliverable to them:
- Requirements baseline and interface definitions
- Architecture decisions and rationale (ADRs) tied to risks/constraints
- Implementation plan with verification hooks (test points, logging)
- Change impact assessments that include test and risk implications
Ops stakeholders turn a build into a repeatable product. Their constraints often surface late unless they are engaged early in release planning and change control.
- Who:
- Manufacturing engineering and production leads
- Process validation owners
- Supply chain / planning and incoming inspection
- Configuration management / release packaging
- Typical focus:
- Manufacturability and process validation needs
- Build/release reproducibility and labeling impacts (e.g., UDI)
- Component availability, lead times, and scalability
- Controlled changes that affect production or distribution
- Typical deliverable to them:
- Release package definition (BOM/configuration baseline, versioning)
- Manufacturing/process validation inputs and acceptance criteria
- Labeling/UDI impact summary (as applicable)
- Supply chain risk items and change notifications
Service / Support / Training is where “release readiness” becomes real. They determine whether the product can be installed, supported, and troubleshot without creating risk or uncontrolled workarounds.
- Who:
- Field service and technical support
- Customer success / implementation teams
- Training, IFU, and enablement owners
- Typical focus:
- Troubleshooting workflows and escalation thresholds
- Training burden and IFU clarity
- Installation, upgrade, rollback, and support tooling
- Operational readiness and monitoring runbooks
- Typical deliverable to them:
- Support playbooks, runbooks, and escalation paths
- Installation/upgrade/rollback procedures and release notes
- Training plan, materials, and IFU updates
- Known issues list and troubleshooting decision trees
External parties create real constraints. Their change notifications, quality agreements, and security posture can drive rework and evidence refresh.
- Who:
- Critical component suppliers (libraries, OS vendors, cloud providers)
- Contract manufacturers
- Design partners and integration partners
- Typical focus:
- Quality agreements and change notification rules
- Lead times, obsolescence, and dependency risk
- Vulnerability disclosures and patching constraints
- SLA/uptime commitments and integration readiness
- Typical deliverables to them:
- Requirements and interface specifications for integration
- Quality agreement inputs and change notification expectations
- Security and vulnerability handling expectations (incl. disclosure timing)
- Joint release readiness checklist (test evidence, environments, dates)
Postmarket (Complaints / CAPA / Surveillance) signals trigger change. This group routes field data into controlled problem resolution, CAPA, and sometimes regulatory reporting.
- Who:
- Complaint handling and vigilance support
- CAPA owners and reliability engineering
- Clinical affairs / medical safety monitoring (as applicable)
- Typical focus:
- Trend signals and escalation rules
- Root cause evidence and recurrence prevention
- Field actions, effectiveness checks, and monitoring updates
- Change triggers that require updated risk and verification evidence
- Typical deliverables to them:
- Complaint trend summaries and signal triage criteria
- RCA package with evidence and contributing factors
- CAPA plan and effectiveness check evidence
- Change-control links back to updated risk and verification evidence
These stakeholders can define acceptance criteria in contracts. They can also impose constraints through cybersecurity questionnaires, interoperability demands, and liability terms.
- Who:
- Customer procurement and value analysis committees
- Customer legal/compliance stakeholders
- Commercial and contracting stakeholders (internal and customer-side)
- Typical focus:
- Contract acceptance criteria and deliverables
- Interoperability and implementation requirements
- Warranty, liability, and support obligations
- Security questionnaires and compliance terms
- Typical deliverables to them:
- Clear acceptance criteria and validation approach for contracts
- Security and compliance responses (questionnaires, attestations)
- Interoperability/integration documentation and implementation plan
- Support and warranty terms mapped to operational capabilities
These are external acceptance authorities. Even when they are not in day-to-day meetings, you must anticipate what evidence they will expect to see and how it will be traced.
- Who:
- Regulators (e.g., FDA)
- Notified Bodies (EU)
- External auditors and inspectors (as applicable)
- Typical focus:
- Sufficiency of objective evidence and traceability
- Risk acceptability rationale and risk control verification
- Change-control discipline and configuration management
- Audit-ready decision records and review approvals
- Typical deliverables to them:
- Traceability and DHF-ready evidence package
- Risk management file with residual risk rationale
- V&V evidence summaries with approvals and deviation dispositions
- Change-control history and configuration baseline records
Use this table as a starting point for your stakeholder register. Tailor it for your product and QMS.
| Stakeholder group | Typical decision rights | Evidence they often own/review | Common “gate” they influence |
|---|---|---|---|
| QA/RA | Process compliance; release sign-off (varies by org) | Design review records, DHF evidence, submission-support evidence | Design reviews; release readiness |
| Risk owners (ISO 14971) | Residual risk acceptability | Risk file updates; risk control verification linkage | Risk review; change control |
| V&V / Test | Test strategy and execution readiness | Protocols, reports, traceability to requirements | V&V readiness; regression scope |
| Clinical / end users | Clinical acceptance; workflow fit | Usability evidence, validation rationale, feedback summaries | Validation readiness; UAT |
| Cybersecurity / privacy | Security controls acceptance | Threat model evidence, security test outputs, SBOM posture | Release readiness; postmarket monitoring |
| Operations / service | Supportability acceptance | Training readiness, service procedures, monitoring runbooks | Release readiness; rollout |
| Postmarket / CAPA | CAPA decisions and escalation | Complaint trends, RCA records, CAPA effectiveness checks | Post-release monitoring; change trigger |
| Engineering (systems/software) | Architecture/design tradeoffs; implementation readiness | Design decisions (ADRs), interface specs, trace links | Architecture/ design reviews; requirements baseline |
| Manufacturing / Operations | Manufacturability and process validation acceptance | Process validation inputs, configuration/release packaging | Operational readiness; release packaging |
| Service / Support / Training | Field readiness acceptance; escalation thresholds | IFU/training materials, support playbooks, runbooks | Release readiness; rollout supportability |
| Suppliers / Partners | Change notifications; dependency and quality constraints | Quality agreements, notifications, component/security posture | Change control; release readiness |
| Customers / Procurement / Legal | Contract acceptance criteria; commercial constraints | Contract deliverables, security questionnaires, compliance terms | Contract deliverables, security questionnaires, compliance terms Contract acceptance; rollout approval |
| Regulators / Auditors | External acceptance constraints (through audits/inspections) | Traceability, risk rationale, V&V evidence, change-control records | Audit readiness; submissions/inspection readiness |
🤖 AI and Machine Learning
If your product uses AI/ML, add stakeholders who own the data, model behavior, and post-release monitoring. In AI/ML systems, “evidence” includes not only software verification, but also model performance claims, validation design, and drift/monitoring controls.

This group builds and changes the model. They are a core stakeholder because model behavior is part of the product’s safety and effectiveness claims.
- Who:
- Data scientists and ML engineers
- Applied research engineers (as applicable)
- Model “owners” (named role in some orgs)
- Typical focus:
- Model design choices and training approach
- Feature engineering and model limitations
- Reproducibility of training runs (data, code, parameters)
- Performance tradeoffs (sensitivity/specificity, calibration)
- Typical deliverables to them:
- Intended use and performance targets (what “good” means clinically)
- Data requirements and labeling guidelines
- Change-control rules for model updates (what can change and how)
- Verification/validation scope that will be used to accept a model update
This group makes sure the training and validation data is trustworthy, lawful to use, and traceable. In regulated environments, this is part of your evidence chain.
- Who:
- Data governance lead / data steward
- Data engineering (pipelines, lineage)
- Labeling operations / annotation teams (internal or vendor)
- Privacy and compliance partners (shared ownership)
- Typical focus:
- Dataset provenance and lineage
- Labeling quality and inter-rater agreement
- Data retention, access controls, and consent constraints
- Bias/fairness risks and subgroup representation
- Typical deliverables to them:
- Data flow diagrams and privacy constraints (what data can be used where)
- Dataset specification (inclusion/exclusion, sources, versioning)
- Labeling protocol and quality metrics
- Audit-ready dataset inventory and trace links to training/validation runs
This group defines what clinically meaningful performance looks like and how to prove it. They help prevent “model works in dev” from becoming “model fails in clinical reality.”
- Who:
- Clinical validation lead
- Biostatisticians / clinical data scientists
- Clinical affairs and subject matter experts (SMEs)
- Typical focus:
- Clinically meaningful endpoints and acceptance criteria
- Validation design (study design, sample size, dataset split rules)
- Subgroup analysis and generalizability
- Clinical risk framing for false positives/negatives
- Typical deliverables to them:
- Model performance report format and statistical analysis plan (SAP)
- Validation datasets and rationale for representativeness
- Results summaries with subgroup breakdowns
- Clear “go/no-go” acceptance criteria for model changes
Some organizations add an explicit oversight layer for algorithms. When it exists, it is a high-leverage governance stakeholder.
- Who:
- Model risk management committee
- Algorithm oversight board
- Safety governance or clinical safety committee representatives
- Typical focus:
- Acceptable performance boundaries and risk tradeoffs
- Monitoring thresholds and escalation rules
- Approval of model update limits and change-control conditions
- Risk acceptability and patient safety impact
- Typical deliverables to them:
- Model “safety case” summary (risks, controls, limitations)
- Monitoring plan and alert thresholds
- Change impact assessment for model updates
- Decision record for approval (including conditions and scope)
This group keeps the model controlled in production. They own “model-in-field” traceability, monitoring, and rollback readiness.
- Who:
- MLOps engineers / platform owners
- Release engineering / DevOps partners
- Site reliability engineers (SRE), where applicable
- Typical focus:
- Deployment controls and versioning (model + code + data)
- Monitoring for drift, data quality, and performance signals
- Incident response, rollback, and containment
- Traceability of what model version ran for which patient/case (as applicable)
- Typical deliverables to them:
- Release package definitions for model artifacts (hashes, version IDs)
- Monitoring dashboards, alerting rules, and runbooks
- Rollback plan and validation evidence for deployment pipeline
- Post-release performance review cadence and decision workflow
Stakeholder analysis

Stakeholder analysis is a structured process. It identifies people who can influence outcomes or are affected by them. It also assesses them and plans how to engage them [3]. In MedTech, that definition is incomplete unless you add one sentence:
Stakeholder analysis must also identify who owns which evidence and which sign-offs.
When to run
Run stakeholder analysis:
- at initiation and early planning,
- at every major phase gate (requirements baseline, architecture/design review, V&V readiness, release readiness),
- whenever scope or risk changes materially,
- after major postmarket signals.
This matches common project lifecycle guidance for stakeholder analysis as a repeated practice rather than a one-time exercise [3].
What to learn
For each key stakeholder group:
- Interests: what they value (safety, time-to-market, usability, compliance, cost, reputation)
- Influence: formal decision rights and informal influence
- Attitude: supportive / neutral / resistant
- Evidence responsibility: what they must review/approve (requirements, risk acceptability, V&V outputs, labeling/training)
- Constraints they carry: regulatory expectations, SOPs, resource limits, lead times, external deadlines
Expectation → Evidence
This is the conversion pattern that makes stakeholder management auditable. Stakeholders expect to receive a given Benefit, that creates an expectation from the project. It is important then to agree early on on an Acceptance Criteria that can be delivered as Objective Evidence to the stakeholders involved.
Conversion chain

- Stakeholder expectation → testable acceptance criteria
- Acceptance criteria → traceable requirement(s)
- Requirement(s) → verification method (inspection/analysis/test) + protocol
- Execution → test results + deviations handled
- Review/approval → objective evidence
- Evidence + risk acceptability + approvals → release readiness
IEC 62304 forces this pattern at system scale [1]. Requirements must be testable and traced. Verification and validation must be documented. Changes must trigger updated risk analysis and verification when appropriate. This is consistent with ISO 13485 style design controls [4].
Why it works
This works because it makes alignment observable and testable early:
- It converts “opinions” into measurable acceptance criteria, so stakeholders can agree before implementation.
- It produces traceable requirements, so decisions survive team changes, audits, and late questions.
- It connects each requirement to a verification method and planned evidence, so V&V effort is predictable.
- It assigns the right reviewers and approvers at the right time, which reduces decision churn and review bottlenecks.
- It keeps changes controlled, because impact is evaluated against requirements, risk, and evidence before release.
On the other hand, when expectations remain implicit, disagreement is delayed until the most expensive time:
- “This isn’t what I meant”
- “We need additional testing”
- “Regulatory needs a rationale”
- “Ops can’t support this”
- “Clinical workflow won’t accept this UI”
⚠️ Failure Patterns
- Acceptance criteria are subjective. Examples are “easy to use,” “fast,” or “safe” without measurable definition.
- When requirements are missing measurable criteria (they cannot be verified)
- When evidence exists but is not reviewed/approved by the correct decision owner
- Software Changes stay just in the code for too long. They are not propagated through traceability, risk, and V&V artifacts.
Toolkit
Stakeholder register
At minimum, capture:
- stakeholder/group name
- role and decision rights (who approves what)
- interest/value driver
- influence (formal + informal)
- current attitude
- engagement approach (what works)
- evidence ownership: what they must review/approve
- cadence + triggers (what events require engagement)
Mapping tools
Use the simplest tool that answers the decision:
- Power–interest grid: fast triage
- Engagement assessment matrix: current vs desired engagement levels. For example: unaware → resistant → neutral → supportive → leading [5]
- Influence mapping: coalitions and dependency paths
Engagement plan
A stakeholder engagement plan should explicitly include:
- engagement objectives per segment (reduce rework, accelerate approvals, improve adoption)
- cadence + event triggers (change requests, nonconformities, audit findings, postmarket signals)
- forums for decisions (design reviews, risk reviews, release readiness reviews)
- escalation thresholds and response time expectations
- how stakeholder inputs become tracked actions (and how they are verified/closed)
Evidence + Decision loop
Treat stakeholder engagement like a system. Run it whenever reality changes.
The loop (6 steps)

- Name the trigger Examples: change request, defect trend, audit finding, clinical feedback, supplier notification.
- Identify affected stakeholders Separate: inform vs decide vs approve.
- Translate impact into evidence work What must be updated/re-tested/re-approved? Traceability? Risk file? Labeling? Training? Cybersecurity documentation?
- Re-align on risk + acceptance What is now acceptable, and why? Who must accept residual risk?
- Decide Continue / pivot / pause / stop (or approve with conditions).
- Record (audit-ready) Capture the decision, rationale, evidence reviewed, and updated artifacts.
This is compatible with PMI’s value delivery framing [2]. Decisions should produce outcomes that are worth the effort and expense. Stakeholders define what “worth it” means.
Example: late change
Scenario: A clinical stakeholder requests a UI change. It affects how dose recommendations are displayed. The change looks “small.” It still touches safety and usability.
Run the Evidence + Decision loop:
- Trigger: late change request affecting dose display.
- Affected stakeholders: Clinical, QA/RA, Risk owners, V&V, Cybersecurity/privacy (if logging/telemetry changes), Ops/service (training).
- Evidence impact (typical):
- Update acceptance criteria and requirements (traceable).
- Update risk analysis: hazard sequence, risk controls, residual risk rationale.
- Update V&V scope: regression tests, UI/usability evidence, updated protocols/reports.
- Update labeling/training if user workflow changes.
- Update release notes and configuration baseline.
- Re-align on risk + acceptance: confirm whether risk is reduced or introduced. Confirm who must sign.
- Decision: approve change with evidence conditions (or defer to next release).
- Record (audit-ready): change request, impact assessment, approvals, updated trace links, and test evidence.
Key lesson: the cost of late change is rarely coding time. It is usually evidence re-validation time.
Proactive RCA
The name of the game is prevention, don’t be a firefighter.
Use proactive Root Cause Analysis (RCA) to keep stakeholder engagement signal-driven instead of crisis-driven. The goal is to prevent repeat incidents by converting early signals into preventive, evidence-backed changes [6]. A proactive culture looks for early signals and uses structured RCA to prevent repeated incidents.
When to trigger it
Use this when you see a repeating or rising signal, for example:
- complaints / postmarket trends
- near-misses
- recurring defects or deviation themes
- review bottlenecks that repeatedly delay approvals
What it produces
Done well, proactive RCA turns “symptoms” into system constraints and then into controlled updates:
- clearer requirements and acceptance criteria
- updated risk controls and risk rationale
- updated verification methods and test coverage
- updated monitoring signals and operational controls (training/process updates)
Why it helps
- Signals become formal triggers for the Evidence + Decision loop (see previous section), so the right decision owners engage early.
- RCA forces a shift from what happened to why the system allowed it, which prevents recurring evidence debt and late rework.
Lightweight workflow

- Detect a repeating signal (trend, theme, or near-miss)
- Write a measurable problem statement (scope, frequency, impact)
- Investigate with evidence (logs, traceability, test results, complaints, CAPA data)
- Confirm root cause (avoid “single-point blame”; capture contributing factors)
- Implement a preventive fix (requirements/risk/process/test changes)
- Verify + standardize (prove effectiveness; update monitoring, training, and SOPs) [6]
Stakeholders and IEC 62304
IEC 62304 is a software life cycle standard. It is risk-driven and it tells you what processes and work products must exist to develop and maintain medical device software in a state of control [1].
It does not list job titles. Instead, it creates obligations that someone must own:
- plans must be defined and followed,
- requirements and architecture must be documented and reviewed,
- verification/validation evidence must be produced and approved,
- configuration and change control must be enforced,
- problems found in development or in the field must be resolved and fed back into risk and maintenance.
That is why IEC 62304 implicitly defines stakeholder needs. If you accept IEC 62304, you are accepting that the project requires:
- decision owners (who can approve/reject evidence and residual risk), and
- evidence owners (who produce, review, and maintain objective evidence).
This section explains how to convert “IEC 62304 requires X” into “these stakeholders must be engaged.”

How to read this mapping
Think in three layers:
- Process obligation (IEC 62304): what must be controlled.
- Evidence artifact: what gets produced (plan, requirement, test report, change record, problem report).
- Stakeholder role: who must review/approve/operate that evidence.
Practical mapping
This section explains how IEC 62304 was incorporated into stakeholders mapping section above.
- QA/RA(design controls + audit readiness)
- Why they appear in 62304 terms: IEC 62304 assumes controlled processes, records, and approvals [1].
- What they own: process adherence, document control, review packages, audit-ready traceability.
- Risk management owners (ISO 14971)(residual risk acceptance)
- Why they appear in 62304 terms: risk controls must become requirements and must be verified [1].
- What they own: risk acceptability decisions, linkage between risk controls → requirements → verification evidence.
- V&V / Test / Quality Engineering(objective evidence production)
- Why they appear in 62304 terms: verification/validation must be planned, executed, and documented [1].
- What they own: protocols, reports, coverage, deviation handling, approval throughput.
- Engineering (software/systems)(requirements + architecture + implementation)
- Why they appear in 62304 terms: requirements and architecture/design must be defined, implemented, and maintained under change control [1].
- What they own: design decisions, traceability hooks, implementation changes and their impact.
- Configuration management / release engineering(baselines + reproducibility)
- Why they appear in 62304 terms: configuration management is a required support process [1].
- What they own: versioning, baselines, build/release integrity, reproducible releases.
- Operations / Service (release readiness + supportability)
- Why they appear in 62304 terms: maintenance and problem resolution require operational readiness and controlled updates [1].
- What they own: training readiness, support procedures, monitoring runbooks, deployment constraints.
- Postmarket / Complaints / CAPA (field signals → controlled change)
- Why they appear in 62304 terms: problem resolution and maintenance are triggered by issues found in the field [1].
- What they own: signal triage, RCA/CAPA routing, escalation rules, feedback into risk and change control.
One obligation, many stakeholders

If IEC 62304 requires “problem resolution,” a single field issue typically touches:
- Postmarket (signal triage)
- Engineering (root cause + fix)
- Risk owners (risk impact)
- V&V (verification scope)
- QA/RA (approval + records)
- Ops/Service (rollout + monitoring)
AI/ML-enabled devices: stakeholder additions and shifts
AI/ML doesn’t remove the IEC 62304 pattern. It expands it. You still need traceable requirements and objective evidence. You also need to manage data, model behavior, and post-release performance drift as first-class sources of risk.
- Data science / ML engineering: owns model design choices, training runs, and reproducibility (data, code, parameters).
- Data management / data governance: owns dataset provenance, labeling quality, privacy constraints, and data retention rules.
- Clinical validation / biostatistics: defines clinically meaningful performance targets, validation design, and subgroup analysis expectations.
- Model risk management / algorithm oversight (where present): reviews safety cases for models, change limits, and monitoring thresholds.
- MLOps / model operations: owns deployment controls, monitoring, incident response, rollback, and traceability of “model-in-field” versions.
- Human factors / usability (for AI outputs): ensures the AI’s outputs are interpretable and do not drive unsafe use errors.
- Security (expanded): threat modeling includes model supply chain, data poisoning risks, and protected model artifacts.
What changes in “evidence” for AI/ML
- You need evidence not only that the software meets requirements, but that the model meets performance claims on defined data and stays inside defined operating conditions.
- You need a clear change-control story for model updates (what can change, how it is validated, and how it is approved).
Practical stakeholder implications

- Add “dataset owner” and “model owner” roles to your stakeholder register (with explicit decision rights).
- Treat model updates as change-control events. Always link them to risk, verification/validation scope, and release readiness artifacts.
Evidence debt

IEC 62304 is built around controlled, traceable evidence. That means work moves through people and approvals, not just through code. Requirements are reviewed. Risks are accepted. Tests are approved. Releases are signed off.
When you change requirements late, you are not only changing code. You are often invalidating previously approved evidence. That forces rework across stakeholders (QA/RA, Risk owners, V&V, Engineering, Ops). The “redo cost” created by those repeated review cycles is what I mean by evidence debt.
This is why evidence debt belongs in a stakeholder article. The cost is not mainly engineering effort. The cost is coordination + re-approval + re-verification across the acceptance authorities who make IEC 62304 real.
Every late requirement change has an evidence multiplier. Late risk discovery also has an evidence multiplier:
- rework requirements and traceability
- update risk controls and rationale
- rerun verification, sometimes validation
- update labeling/training
- update submissions or technical documentation when applicable
PMI layer
This section keeps the article aligned with PMI language without changing the MedTech-first model.
PMI framing
- Stakeholders are a performance domain
- Projects exist to create value (financial and nonfinancial), and value is perceived differently by stakeholders [2].
- Project success is a consensus view across intended beneficiaries, other stakeholders, and participants.
- Each stakeholder has a list of benefits that they expect from a project.
- Stakeholder engagement is continuous dialogue [2]. It captures feedback. It maintains alignment. It builds credibility.
PMI artifacts
- Stakeholder register → add decision rights + evidence ownership
- Stakeholder analysis → add release-blocking power + risk-acceptance authority
- Engagement assessment matrix → use for approval readiness and adoption readiness [5]
- Stakeholder engagement plan → integrate with design reviews, risk reviews, V&V gates, change control
- Communications plan → keep distinct from engagement (push/pull information flows)
PMBOK 8 – Process Spine

Use PMI process language while executing the MedTech Evidence and Decision loop:
- Identify stakeholders
- Plan stakeholder engagement
- Plan communications management
- Manage stakeholder engagement
- Manage communications
- Monitor stakeholder engagement
- Monitor communications [5]
ESG lens
Environmental, Social, Governance (ESG) connects to stakeholder management because the Social and Governance dimensions are fundamentally about:
- transparency,
- accountability,
- and credible engagement with those affected by decisions.
ESG reporting is often a communication mechanism to build trust. A stronger move is using ESG thinking to make stakeholder value explicit [7]. Examples include patients/users, workforce, regulators, and communities. It also helps you decide what matters most. This is materiality.
A practical MedTech interpretation:
- E (Environmental): device lifecycle impacts, supply chain, sustainability commitments (where applicable)
- S (Social): patient safety, usability, accessibility, equity, workforce impacts
- G (Governance): decision rights, change control, auditability, conflict-of-interest management
Use ESG as a lens to ensure you are not optimizing time-to-market at the expense of long-term trust.
Metrics
Choose metrics that improve decisions rather than punish individuals:
- Decision latency: issue raised → decision made
- Review throughput: time to approve evidence (a common hidden bottleneck)
- Rework due to late objections: number of rework cycles caused by late stakeholder inputs
- Gate readiness predictability: planned vs actual approval dates (requirements baseline, V&V readiness, release readiness)
- Postmarket signals: complaint trends, deviation and CAPA aging, recurring defect themes
References
[1] International Electrotechnical Commission. (2006). IEC 62304:2006 — Medical device software – Software life cycle processes. https://webstore.iec.ch/en/publication/6792
[2] Project Management Institute. (n.d.). A guide to the project management body of knowledge (PMBOK® Guide) – Eighth edition. https://www.pmi.org/standards/pmbok
[3] Six Sigma DSI. (n.d.). Stakeholder analysis. https://sixsigmadsi.com/glossary/stakeholder-analysis/
[4] U.S. Food and Drug Administration. (2024). Quality management system regulation (QMSR): Design and development [PDF]. https://www.fda.gov/media/189041/download
[5] Project Engineer. (n.d.). Project stakeholder management according to the PMBOK. https://www.projectengineer.net/project-stakeholder-management-according-to-the-pmbok/
[6] International Organization for Standardization. (2019). ISO 14971:2019 — Medical devices – Application of risk management to medical devices. https://www.iso.org/standard/72704.html
[7]Elite Asia. (n.d.). Stakeholders + ESG framework. https://www.eliteasia.co/esg-main-solution/







Leave a Reply